
The Silent Heart Crisis: Insights from the Recent MASALA Study Report
By Dr. Kavitha Reddy
The MASALA Study, published in the popular medical journal, has issued a wake-up call for the South Asian community in the United States. The research reveals a startling health disparity: South Asian adults are developing critical risk factors for heart disease—such as prediabetes, type 2 diabetes, and high blood pressure—significantly earlier than white, Black, Hispanic, and Chinese Americans.
 The MASALA Study (Mediators of Atherosclerosis in South Asians Living in America): This study specifically tracks South Asian individuals who trace their ancestry to Bangladesh, India, Nepal, Pakistan, or Sri Lanka. The researchers analyzed health data from approximately 2,700 adults between the ages of 45 and 55.
The MASALA Study (Mediators of Atherosclerosis in South Asians Living in America): This study specifically tracks South Asian individuals who trace their ancestry to Bangladesh, India, Nepal, Pakistan, or Sri Lanka. The researchers analyzed health data from approximately 2,700 adults between the ages of 45 and 55.
Even more confounding is the “South Asian Paradox”: these elevated risks persist despite South Asian adults often maintaining “healthier” lifestyle markers, including higher-quality diets and lower alcohol consumption, compared to other ethnic groups. This research suggests that for this population, the biological clock for cardiovascular health moves faster, necessitating a radical shift in how we approach screening and prevention.
Unpacking the Data
Atherosclerosis is the slow, progressive buildup of fat, cholesterol, and other substances (plaque) in the artery walls, causing them to thicken, harden, and narrow. This accumulation limits oxygen-rich blood flow to tissues and can cause blood clots. It is the underlying cause of most cardiovascular diseases, including heart attacks and strokes.
By analysing these datasets, researchers were able to pinpoint exactly when and how heart disease risk factors begin to diverge across different ethnicities. The results showed that by the time South Asians reach their mid-40s, the seeds of future heart disease—specifically Atherosclerotic Cardiovascular Disease (ASCVD)—have already been sown at rates far higher than their peers.
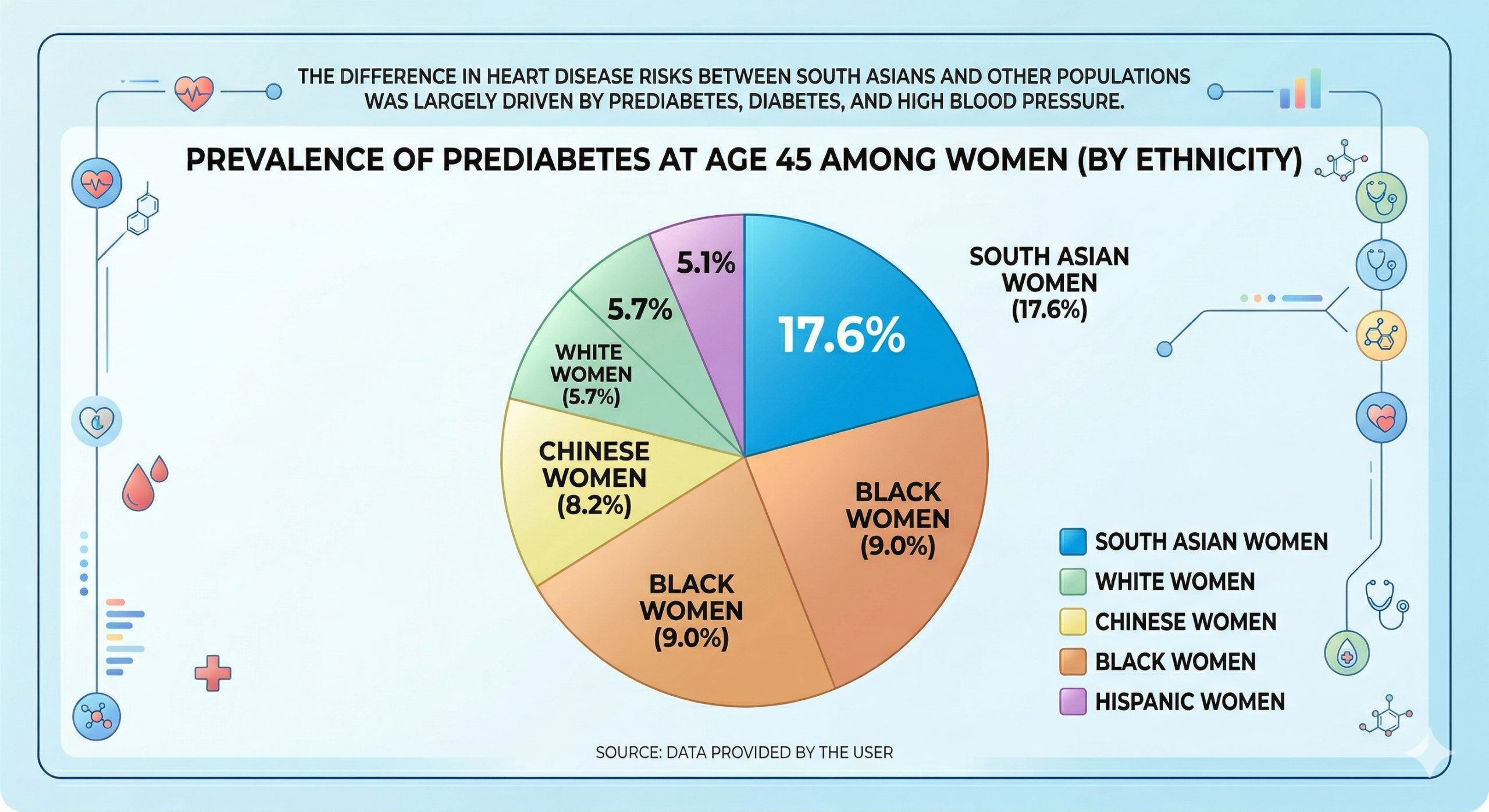
The Prediabetes Explosion
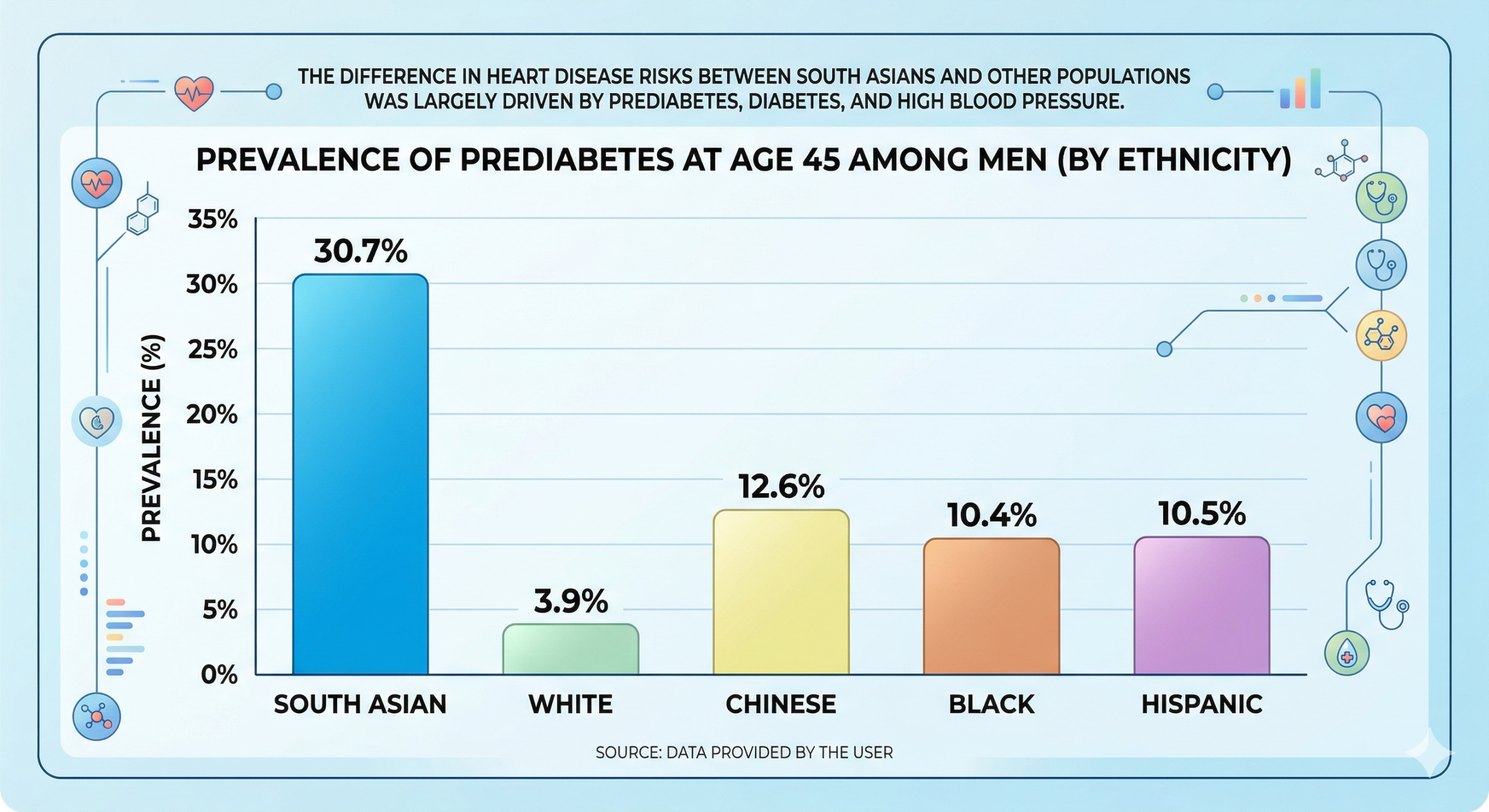
The most dramatic finding in the report involves blood sugar management. At age 45, the disparity in prediabetes prevalence is staggering. Prediabetes is a condition where blood sugar levels are higher than normal but not yet high enough to be classified as type 2 diabetes; however, it is a major precursor to heart attacks and strokes.
| Ethnic Group (Age 45) | Men (Prediabetes %) | Women (Prediabetes %) |
|---|---|---|
| South Asian | 30.7% | 17.6% |
| White | 3.9% | 5.7% |
| Chinese | 12.6% | 8.2% |
| Black | 10.4% | 9.0% |
| Hispanic | 10.5% | 5.1% |
As the data shows, “South Asian men at age 45 are nearly eight times more likely to have prediabetes than white men. South Asian women fare better than the men but still face nearly three times the risk of their white female peers. By age 55, these numbers translate into a high conversion rate to Type 2 diabetes, with South Asian adults being at least twice as likely to have the disease compared to white adults of the same age.”
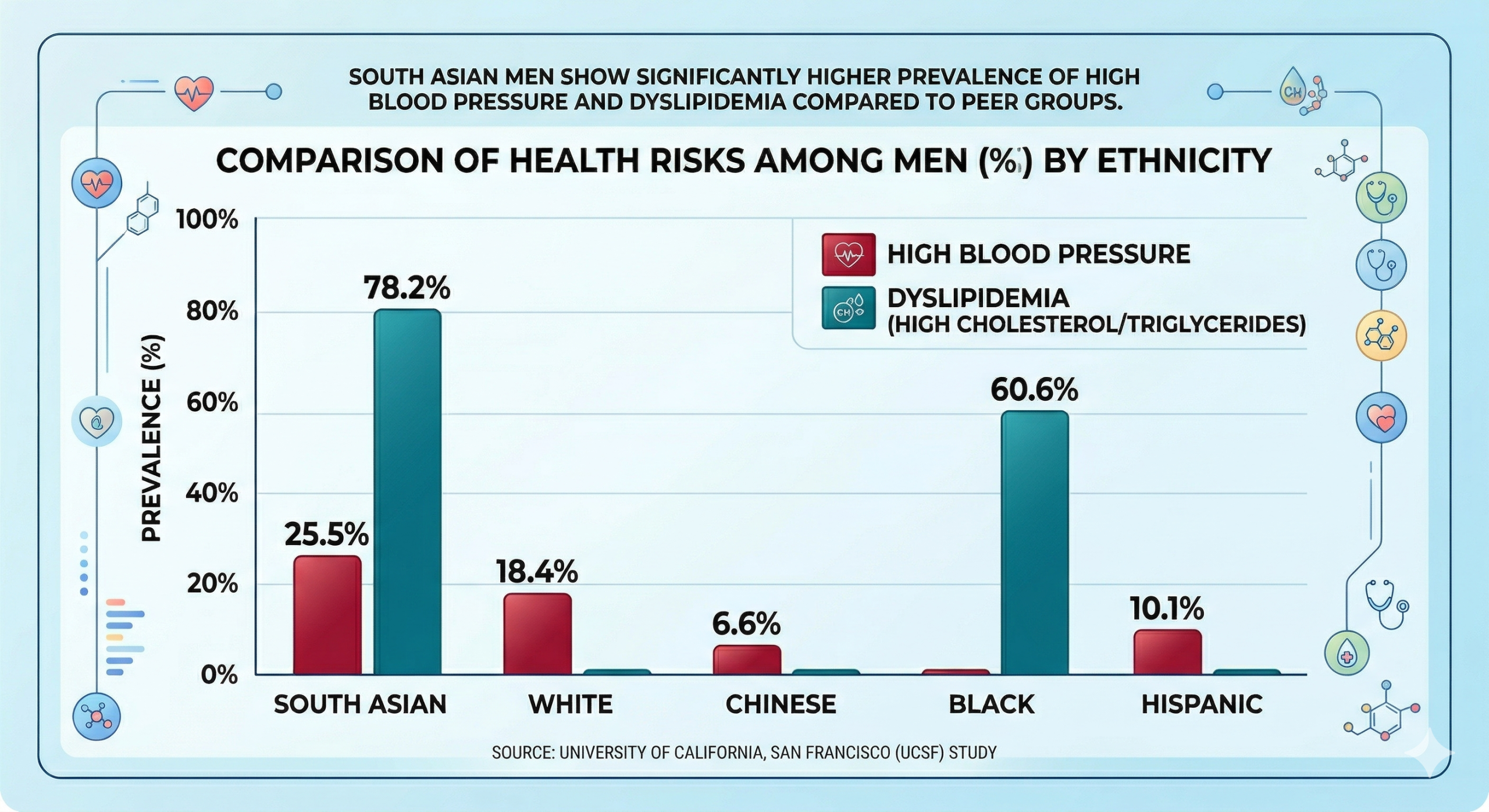
Hypertension and Cholesterol: The Silent Pressures
High blood pressure (hypertension) and dyslipidemia (unhealthy levels of cholesterol or triglycerides) are the “silent killers” that contribute to plaque buildup in the arteries. The study found that:
- Hypertension: South Asian men had a much higher rate of high blood pressure (25.5%) than white (18.4%), Chinese (6.6%), and Hispanic men (10.1%).
- Dyslipidemia: When compared to Black men, South Asian men had a much higher prevalence of high cholesterol and triglycerides (78.2% vs. 60.6%).
What makes these findings particularly striking is the comparison to Black adults. Historically, Black Americans have faced the highest rates of hypertension in the U.S. due to a mix of systemic, environmental, and genetic factors. This study found that South Asians have “similar or slightly lower” rates of high blood pressure than Black adults, placing them in one of the highest-risk categories in the country.
The “South Asian Paradox”: Healthy Habits, High Risk
One of the most persistent myths in cardiovascular health is that heart disease is purely a result of “poor choices”—lack of exercise, excessive drinking, or a high-fat diet. This study shatters that narrative for the South Asian community.
The researchers used the American Heart Association’s “Life’s Essential 8” metrics to measure lifestyle behaviors. They found that South Asian adults actually reported:
- The best quality diets among all groups studied.
- Lower alcohol consumption (defined as one or more drinks per week).
- Comparable exercise levels to other ethnic groups.
This situation creates a medical paradox. Why are people with better diets and lower alcohol use getting sick earlier? While the study doesn’t provide a definitive answer, experts point toward a combination of genetic predisposition and ectopic fat deposition. South Asians tend to store fat around internal organs (visceral fat) even at a lower Body Mass Index (BMI), which can trigger insulin resistance and inflammation much earlier than in other populations.
Redefining Prevention: Screen Early, Screen Often
The implications of this study are clear: the standard “waiting game” in American medicine must end for South Asian patients. Traditionally, many screenings for cholesterol and blood sugar begin in the late 40s or 50s. For South Asians, the wait may be a decade too late.
Senior study author Dr. Namratha Kandula, a professor of medicine at Northwestern University, emphasizes that early detection is the only way to blunt the curve of heart disease.
“If you are a South Asian adult, maintain a healthy lifestyle and undergo screened sooner—monitor blood pressure, glucose/A1c levels, and cholesterol in early adulthood rather than waiting for symptoms.”
Dietary Adjustments
While South Asians often have high-quality diets (including many vegetables and lentils), the American Heart Association suggests specific cultural modifications to further lower risk:
- Swap the Grains: Increase intake of whole grains over refined white rice and flour.
- Oil Selection: Use cooking oils lower in saturated fats (like olive or avocado oil) instead of ghee or palm oil.
- Cooking Methods: Avoid deep-frying foods, which is common in many traditional South Asian appetizers and snacks.
Study Limitations and Future Research
While the findings are robust, the researchers noted several limitations. The data relied partly on self-reported behaviors, which can be subject to memory errors or “social desirability bias” (where participants report what they think the doctor wants to hear). Additionally, participants in the MASALA and MESA studies tended to have higher socioeconomic and educational status, meaning the risks might be even higher in underserved South Asian communities.
There was a ten-year gap between the start of the MESA study (2000–2002) and the start of the MASALA study (2010–2013). However, even with these variables, the trend is undeniable: the South Asian population in the U.S. is facing a unique, early-onset cardiovascular crisis.
“Heart disease does not discriminate, but it does follow different timelines for different people. For South Asian Americans, the message is one of urgency.” By recognizing that “standard” health metrics may not provide a complete picture, and by promoting screenings as early as the 20s or 30s, individuals can proactively manage their cardiovascular health before irreversible damage occurs.
The South Asian Heart Health Advocacy Checklist
1. Essential Lab Tests (The “Big Three”)
Don’t wait for age 45 or 50. If you are South Asian, these should ideally be baselined in your 20s or 30s.
- [ ] Lipid Panel (with Fractionation): Ask for a full breakdown of HDL, LDL, and especially triglycerides.
- Note: South Asians often have a “low HDL/high triglyceride” profile even if total cholesterol looks “normal.”
- [ ] HbA1c & Fasting Glucose: Because the study shows a 30.7% prediabetes rate in men by age 45, you need to know your 3-month blood sugar average (A1c) early.
- [ ] Lipoprotein(a) or Lp(a): This is a genetic protein often elevated in South Asians that isn’t included in standard cholesterol tests. It is a major independent risk factor for early heart attacks.
2. Physical Measurements
- [ ] Blood Pressure Check: Ensure the cuff is the correct size. If your reading is consistently above 120/80, discuss a management plan immediately.
- [ ] Waist-to-Hip Ratio: BMI (Body Mass Index) can be misleading for South Asians. We often carry “visceral fat” around the organs despite having a “normal” weight. A waist measurement of >90 cm (35 in) for men or >80 cm (31 in) for women indicates a higher risk.
3. Advanced Screening (If Risk Factors Exist)
If you have a family history of early heart disease, ask your doctor about:
- [ ] CAC Score (Calcium Scan): A non-invasive CT scan that looks for actual plaque buildup in the heart arteries.
- [ ] High Sensitivity C-Reactive Protein (hs-CRP): A blood test that measures “silent” inflammation in the body.
4. Strategic Questions for Your Doctor
- “I identify as South Asian. Are you using the AHA/ACC Ethnicity Modifier when calculating my 10-year cardiovascular risk score?”
- “Since South Asians have higher rates of diabetes at lower BMIs, should we lower the threshold for my ‘healthy’ weight range?”
- “Based on my family history and these study findings, should we start statin therapy or blood pressure medication sooner than standard guidelines suggest?”
Summary Table: Targets to Aim For
| Metric | Goal for South Asian Adults |
|---|---|
| Blood Pressure | < 120/80 mmHg |
| HbA1c | < 5.7% |
| Fasting Glucose | < 100 mg/dL |
| LDL Cholesterol | < 100 mg/dL (or lower if other risks exist) |
| Triglycerides | < 150 mg/dL |
Since the MASALA study highlighted that South Asian adults often have high-quality diets yet still face elevated risks, the secret isn’t necessarily eating “less”—it’s about changing the biochemical impact of traditional ingredients.
The South Asian diet is often high in “accompanying” carbohydrates (white rice and naan) and inflammatory fats (ghee and palm oil) that can spike blood sugar and triglycerides. Here is a culturally tailored guide to swapping ingredients while keeping the flavors you love.
The South Asian Heart-Health “Smart Swap” Guide
1. The Grain Exchange (Lowering the Glycemic Index)
The goal here is to prevent the massive insulin spikes that lead to the 30.7% prediabetes rate seen in the study.
| Instead of… | Try… | The Health “Win” |
|---|---|---|
| White Basmati Rice | Brown Basmati or Quinoa | Higher fiber slows sugar absorption. |
| Maida (White Flour) Naan | Missi Roti (Chickpea/Besan flour) | More protein and a lower glycemic index. |
| Puffed Rice (Mamra) | Roasted Makhana (Foxnuts) | Higher in magnesium and lower in simple carbs. |
2. The Fat Foundation (Reducing Inflammation)
South Asian cooking often relies on fats that are high in saturated content, which contributes to the higher dyslipidemia (cholesterol) rates found in the research.
| Instead of… | Try… | The Health “Win” |
|---|---|---|
| Ghee or Butter | Extra Virgin Olive Oil or Avocado Oil | Replaces saturated fat with heart-healthy monounsaturated fats. |
| Coconut Milk (Canned) | Greek Yogurt or Nut Pastes | Reduces saturated fat while adding a protein boost. |
| Palm Oil (Vanaspati) | Mustard Oil or Rice Bran Oil | Better omega-3/omega-6 balance for artery health. |
3. The Protein & Prep Shift
Because South Asians often have a “normal” BMI but high internal (visceral) fat, increasing protein-to-carb ratios is essential.
- Deep Frying vs. Air Frying: Instead of deep-frying Samosas or Pakoras, use an air fryer or bake them. This can reduce calorie density by up to 70% without losing the crunch.
- Lentils (Dal) Optimization: Dal is great, but it is often 70% carbohydrate.
- The Swap: Add a handful of spinach (Palak) or methi to every dal dish to increase volume and fiber without adding carbs.
The “Plate Method”: Traditional plates are often 70% rice/roti and 30% veg/dal. Flip it: Fill 50% of your plate with non-starchy vegetables (okra/bhindi, karela, or cauliflower), 25% with protein (dal, paneer, tofu, or fish), and only 25% with grains.
Flavor Without the Salt (Managing Hypertension)
The study noted high blood pressure is a major risk factor. South Asian pickles (Achaar) and spice blends often hide massive amounts of sodium.
- Spice over Salt: Use more Amchur (dried mango powder), Kokum, or Fresh Lemon/Lime to get a “tangy” hit that mimics the satisfaction of salt.
- The Achaar Alternative: If you love pickles, try making a “Quick Pickle” at home using fresh ginger, green chilies, and lemon juice with zero added salt or oil.
- Garlic & Turmeric: Both have natural anti-inflammatory and mild blood-pressure-lowering properties. Double the amount you use in your Tadka (tempering)!
A Note on “Cheat” Meals
“You don’t have to give up Mithai (sweets) forever. However, the study shows that South Asians are uniquely sensitive to sugar. Try switching to Stevia-based home-made desserts or using dates/figs for sweetness instead of refined white sugar”.
This 3-day meal plan is designed specifically to address the risks highlighted in the study—high prediabetes rates and early-onset hypertension—while maintaining the traditional flavors of a South Asian kitchen.
The focus is on lowering the Glycemic Index (GI), increasing fiber, and using heart-healthy monounsaturated fats.
3-Day South Asian Heart-Healthy Meal Plan
Day 1: The “Fiber-First” Focus
Goal: Stabilize blood sugar and reduce the 30% prediabetes risk.
- Breakfast: Oats Upma. Swap semolina (suji) for steel-cut oats. Sauté with mustard seeds, curry leaves, ginger, and a double portion of colorful vegetables (carrots, peas, beans).
- Lunch: Ragi (Finger Millet) Roti & Palak Dal. Two Ragi rotis served with a large bowl of yellow moong dal loaded with fresh spinach.
- Side: A large cucumber and tomato kachumber salad with lemon and black pepper (no added salt).
- Snack: A small handful of roasted Makhana (foxnuts) seasoned with turmeric and a dash of olive oil.
- Dinner: Grilled Tandoori Fish or Paneer. Marinated in Greek yogurt and spices, served with a massive portion of Baingan Bharta (roasted eggplant) and only a half-cup of brown basmati rice.
Day 2: The “Protein-Power” Shift
Goal: Reduce visceral fat by increasing protein-to-carb ratios.
- Breakfast: Moong Dal Chilla (Lentil Crepe). Made with soaked and ground split yellow moong dal, topped with grated paneer and finely chopped onions/chilies.
- Lunch: Chickpea (Chole) Salad. Use boiled chickpeas mixed with chopped bell peppers, onions, tomatoes, and a dressing of olive oil and amchur (mango powder).
- Swap: Skip the Bhatura/Puri; eat the chickpeas as a hearty salad or with a small portion of quinoa.
- Snack: One small seasonal fruit (like a pear or a small apple) and 5 soaked almonds.
- Dinner: Mixed Vegetable Sabzi (Bhindi or Gobi). Cooked in mustard oil with minimal salt.
- Grain Swap: Missi Roti (made with a 1:1 ratio of chickpea flour and whole wheat flour) to provide more protein than a standard roti.
Day 3: The “Anti-Inflammatory” Day
Goal: Use traditional spices like turmeric and garlic to support artery health.
- Breakfast: Vegetable Masala Omelet (or Tofu Scramble). Loaded with onions, tomatoes, green chilies, and extra turmeric. Serve with one slice of sprouted grain toast (no butter).
- Lunch: Brown Rice Khichdi with “Double Veg.” Use a 1:1:2 ratio of brown rice to dal to vegetables (cauliflower, beans, and carrots). Temper with cumin and garlic in a teaspoon of avocado oil.
- Pro Tip: Serve with a side of homemade flaxseed (alsi) chutney for Omega-3 benefits.
- Snack: Sprouted Moong Salad. Steamed sprouts with a squeeze of lime and chaat masala.
- Dinner: Methi (Fenugreek) Chicken or Soya Chunks. Fenugreek is excellent for blood sugar management. Serve with a side of Karela (Bitter Gourd) sautéed with onions to help manage glucose levels.
3 Key Rules for Success
- The “Tadka” Transformation: Use only 1–2 teaspoons of oil for tempering. Avoid “floating” oil in your curries.
- The Salt Substitute: Use fresh lemon juice, ginger, and green chilies to provide the “kick” your palate craves, which helps lower your dependence on salt (and manages high blood pressure).
- Water Over Chai: If you drink Masala Chai, use skim or almond milk and zero sugar. Try to drink 2 liters of plain water daily to help with digestion and metabolic health.
Summary of Daily Goals
| Meal Component | Target |
|---|---|
| Vegetables | At least 3–4 cups per day |
| Grains | Limit to 1 cup (cooked) per meal |
| Protein | Include in every single meal |
| Fats | Stick to liquid plant oils (Olive, Mustard, Avocado) |
Even at a normal-looking weight, South Asians face higher risks of diabetes and heart disease, making nutritious foods like vegetables, fruits, and whole grains essential.
Ongoing stress and depression are strongly linked to an increased risk of cardiovascular disease.

Smoking, chewing tobacco, and traditional forms significantly raise the risk of heart attacks and strokes in an already vulnerable population.

Lower muscle mass and higher body fat levels make a combination of aerobic activity and strength training especially important for South Asians.
Heart disease often appears earlier and runs strongly in South Asian families, increasing risk across generations.
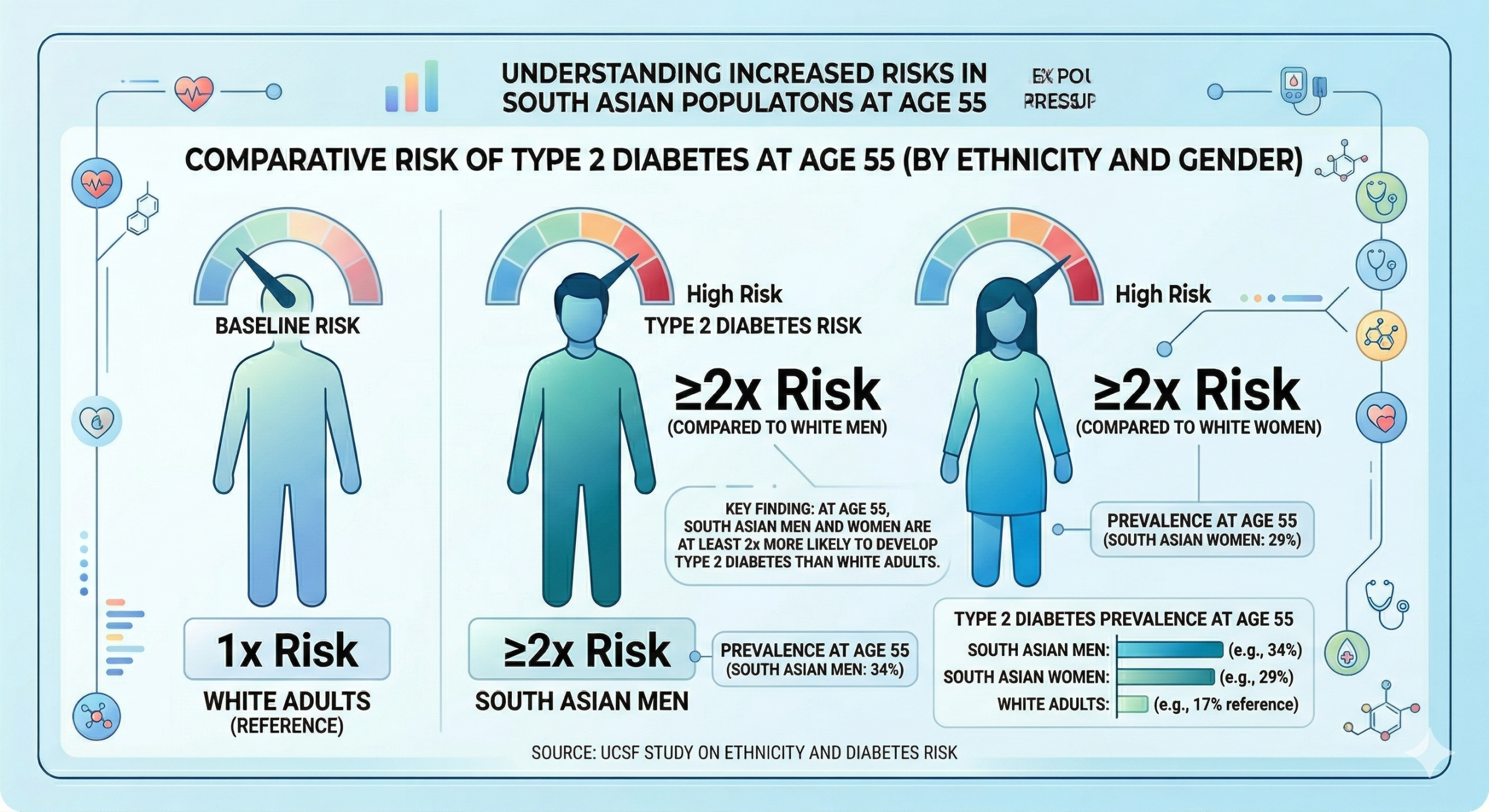
At age 55, both South Asian men and women were at least two times more likely to develop type 2 diabetes when compared to white adults at the same age. Despite having higher rates of heart disease risk factors, South Asian adults also had the best quality diet, lower use of alcohol and comparable exercise habits.
About the Author
Dr. Priya Ramanathan, an Indian-American scientist, holds a Ph.D. in Molecular Biology and has built a distinguished career at the intersection of research and scientific communication. With deep expertise in cellular and molecular sciences, her work has contributed to advancing understanding in key areas of biology. Known for her analytical insight and intellectual rigor, she has earned recognition for her contributions to scientific research and innovation. Her career reflects a rare blend of scientific excellence and thought leadership. She is also a strong advocate for diversity and mentorship in STEM, inspiring the next generation of scientists.












")







